

Let’s skip the part where I pretend you need convincing that ED medication works. You already have the script in hand. What nobody handed you was the user manual, the real one, not the folded paper insert nobody reads. So here’s that manual, written the way I’d actually tell a friend, not the way a pharmacy leaflet does.
One thing up front, and I mean this: I’m not a clinician and I can’t set your dose or your schedule. Nobody but the person who prescribed for you can do that safely, because it depends on your heart, your other meds, your whole picture. What I can do is tell you what the actual research says, what the actual risks are, and where the real line is that you do not cross no matter what. Consider this the harm-reduction version. Not “don’t do this.” Just, “if you’re doing this, do it with your eyes open.”
The part that isn’t a suggestion
I want to put the serious stuff first instead of burying it at the bottom where these articles usually stash it, because burying it is how people get hurt.
PDE5 drugs and nitrate medications do not mix. Full stop. The pharmacology reference is blunt about it: combining sildenafil with nitrates is contraindicated because it can cause a severe, life-threatening crash in blood pressure. Nitrates only become safe again roughly 24 hours after the PDE5 drug clears your system [2]. Nitrates show up a lot in heart medication, especially anything for chest pain. If that’s you, this isn’t a “talk to your doctor about timing” situation. It’s a do-not-combine situation, no exceptions, no “just this once.”
This is also exactly why the intake questions on any legit platform matter, and why lying or skipping through them to get to the checkout screen is the single riskiest thing you can do here. The person setting your dose can only do it safely if they actually know what else is in your body.
One more thing worth knowing while we’re being honest: ED itself is frequently an early signal of cardiovascular trouble, not just its own isolated problem. The American Urological Association’s guideline says men should be counseled about that connection [1]. So the same heart concern that makes the nitrate rule non-negotiable is also a reason to actually get looked at, not just quietly refill a pill forever.
That’s the floor. Everything below this is negotiable with your clinician. That part is not.
Now, the stuff that actually is your call
Here’s where it gets more interesting, because a lot of this dosing conversation genuinely comes down to what fits your life, not just what’s “correct.”
Most people picture ED meds as an on-demand thing: take it, wait, it works for a window, it wears off. But some of these drugs also come in a low daily dose, taken every day regardless of whether you’re expecting to need it, so the medication is just quietly present all the time and timing stops being a thing you have to think about.
These aren’t just two schedules. They’re two different relationships with the drug. On-demand means less total medication over a month, plus some planning around sex. Daily means more total exposure, but a kind of built-in readiness that a lot of people find takes the anxiety out of the equation. Neither one is the “correct” choice. It’s a tradeoff, and it’s genuinely worth having an opinion about when you talk to your prescriber, instead of just taking whatever you were handed by default.
What the research actually shows, which might surprise you
Here’s a piece of information that doesn’t get talked about enough. There’s real head-to-head data on daily versus on-demand tadalafil, and it doesn’t land where people assume.
A meta-analysis in Sexual Medicine pooled long-term studies (24 weeks or more) comparing daily tadalafil against on-demand tadalafil. The daily approach came out ahead on effect, and it also had a lower rate of treatment-emergent side effects than on-demand dosing [3]. Sit with that for a second, because most people’s gut instinct is “less medication in my system, less risk.” In this comparison, that instinct was wrong. The steady daily dose won on both counts.
I’m not telling you daily is the answer for you. The trials pool different men and different studies, and plenty of people do great on-demand and don’t want to take something daily they don’t feel they need every day. But if part of why you chose on-demand was an assumption that it’s automatically gentler, that assumption isn’t backed by this data. Worth raising with whoever prescribed for you.
The numbers, if you want them (and what they don’t tell you)
People always want a milligram figure, so here’s one that’s real. The daily tadalafil studies that established onset and effect used 5 mg once a day [4]. That’s the number that exists in the literature for the daily strategy. It is not a number you should hand yourself. On-demand doses run higher per pill because you’re taking them occasionally instead of continuously, and what’s right for you depends on the drug and your clinician’s read of your situation. I’m not giving you an on-demand chart to self-medicate from, and if anyone hands you one without knowing your history, that’s a red flag, not a shortcut.
The reason for the caution isn’t nervousness for its own sake. It’s that the safe dose depends entirely on things only your prescriber knows, especially your cardiovascular health and every other pill you’re taking.
How fast this actually kicks in
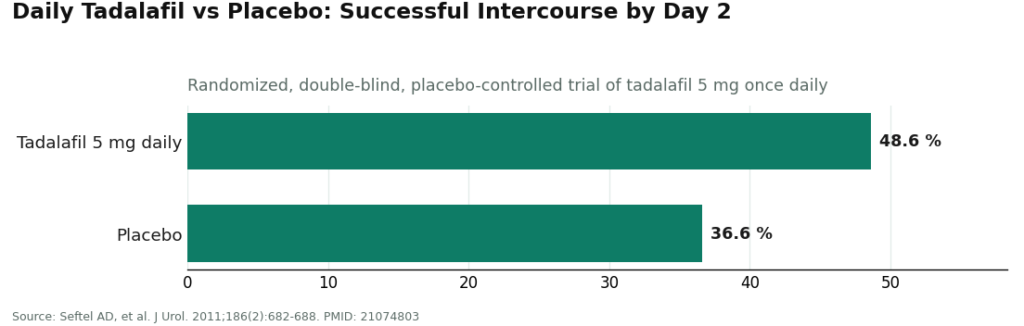
Here’s a number worth knowing if you’re deciding between the two approaches. In a randomized, double-blind, placebo-controlled trial of tadalafil 5 mg once daily, men were already seeing significantly more successful intercourse than the placebo group by day two: 48.6 percent of attempts versus 36.6 percent on placebo [4]. So if you go the daily route, you’re not waiting weeks to know whether it’s doing anything.
For on-demand dosing, the timing works differently. You take it ahead of time, it builds to peak effect over a window, then fades. But the practical lesson is the same either way: don’t judge either strategy off one attempt. Give whatever your clinician set up a real run, and tell them honestly how it’s going instead of silently writing it off after a single try.
Track it. Don’t just wing it and hope.
Here’s something people underrate: dosing isn’t a one-and-done decision, it’s an ongoing back-and-forth. The right rhythm and dose usually get dialed in over a few weeks of paying attention, noticing side effects, noticing what actually works, and telling your clinician the truth about it so they can adjust.
Keeping even a rough log helps more than you’d think. When it was taken, what happened, anything off. That gives your prescriber something real to work with instead of a shrug and “I think it’s fine.” Some supervised telehealth setups build this in directly. FormBlends, for one, offers a tracker app built for exactly this, logging your protocol and how it’s going over time. That’s the low-effort version of a habit that genuinely matters: whatever tool you use, phone notes or an app, track it and be straight with your prescriber about what you actually see.
The short honest version, if you skip everything else
Most ED meds can be taken on-demand or, for some, as a low daily dose, and that choice is a real tradeoff, not a formality. The head-to-head data on tadalafil actually favored daily dosing on both effect and side effects over 24-plus weeks, which is worth bringing up even if you assumed the opposite [3]. The daily studies ran on 5 mg and showed results within about two days, but your actual dose, especially anything on-demand, comes from your clinician, not a chart you found online [4]. And the one rule that overrides everything else here: nitrate medications and these drugs together can crash your blood pressure to dangerous levels, so your prescriber needs to know every heart medication you’re on before any dose gets set [2]. Get the strategy from someone qualified, track how it actually goes, and don’t go quiet if something feels off. That’s the whole game.
Questions people actually ask me
Daily or only when I need it, which is safer? Both are legitimate, they just suit different lives. On-demand means less total medication across a month plus some planning around sex. Daily keeps the drug present in your system so you stop watching the clock. The actual head-to-head research on tadalafil favored daily on both effect and tolerability over 24-plus weeks [3], so don’t assume less-often automatically means safer. Raise it with your clinician either way.
How fast does daily tadalafil actually start working? Faster than most people expect. In a randomized, placebo-controlled trial of tadalafil 5 mg once daily, men saw significantly more successful intercourse than placebo by day two, 48.6 percent of attempts versus 36.6 percent [4]. This isn’t a wait-a-month-to-know situation.
What dose shows up in the actual daily studies? 5 mg once a day is the figure from the trials that established onset and effect for daily tadalafil [4]. That’s context for understanding the strategy, not a number to grab and dose yourself with. On-demand doses run higher per pill, and the right starting point either way is your prescriber’s call, based on your specific situation.
Why does my prescriber need my full heart medication list? Because PDE5 drugs combined with nitrates can cause a severe, life-threatening blood pressure crash, which is why the combination is flatly contraindicated [2]. Nitrates are common in heart medication, especially for chest pain. Your prescriber has to know every cardiac drug you take before setting any dose. This is why intake screening isn’t paperwork, it’s the actual safety mechanism.
One bad attempt, does that mean it’s not working for me? Not by itself. These aren’t one-pill, one-try medications, especially daily dosing where the effect builds over the first several days. Give it a real run, keep a simple log, and tell your clinician the truth so the plan can get adjusted instead of scrapped after one data point.
Why do people keep saying ED can be a heart warning sign? Because it frequently is one, not just a standalone issue. The AUA guideline says men should be counseled about the ED-cardiovascular link [1]. The same heart concern that makes the nitrate rule absolute is a reason the underlying cause deserves real attention, not just a pill to paper over the symptom.
How does an online ED clinic actually work, mechanically?
You fill out a health intake, a licensed physician or nurse practitioner actually reviews it, and if it’s appropriate they write a script that goes to a pharmacy. Usually a few hours to a couple days start to finish, no waiting room involved. The quality of the whole thing hinges on whether that intake form gets a real read or a rubber stamp, and there’s no way to know which from the outside except by how thorough the questions are.
What’s this actually going to cost me?
It swings a lot. A single sildenafil tablet through telehealth can run under a dollar or over twenty, depending on dose, quantity, and brand versus generic. Most platforms tack on a consult fee, sometimes folded into the med price, sometimes not. Insurance almost never touches telehealth ED visits, so plan on paying out of pocket. Compare cost per dose, not the number on the landing page.
Is doing this online actually safe, or am I taking a real risk?
It can be genuinely fine, as long as the clinic does a real medical review and dispenses through a licensed US pharmacy. The medication itself has a long track record. The risk is entirely in skipping the screening. PDE5 drugs and nitrates are a dangerous combination, and a legitimate clinic will ask about heart history, current meds, and blood pressure before approving anything. If a site doesn’t ask, walk away.
How do I actually pick a clinic instead of just guessing?
Look for a real licensed clinician on the review side, a US-licensed pharmacy doing the dispensing, pricing you can see before you enter card info, and an actual way to ask follow-up questions later. If you want something compounded, a custom dose or combination, a physician-supervised compounding pharmacy like FormBlends is a more accountable route than a supplement site or research-chemical seller. Your own health history should drive this decision more than the sticker price does.
References
- Erectile Dysfunction: AUA Guideline. American Urological Association (Burnett AL, et al.), published 2018, amended through 2018. Names FDA-approved oral PDE5 inhibitors as first-line therapy unless contraindicated and identifies ED as a risk marker for cardiovascular disease warranting patient counseling. https://www.auanet.org/guidelines-and-quality/guidelines/erectile-dysfunction-(ed)-guideline
- Smith BP, Babos M. Sildenafil. StatPearls. NCBI Bookshelf (NBK558978). Describes sildenafil as a PDE5 inhibitor used as first-line oral ED therapy and states that coadministration with nitrates is contraindicated because the combination can cause severe, life-threatening hypotension, with nitrate use considered safe only after roughly 24 hours. https://www.ncbi.nlm.nih.gov/books/NBK558978/
- Zhou Z, Chen H, Wu J, Wang J, Zhang X, Ma J, Cui Y. Meta-Analysis of the Long-Term Efficacy and Tolerance of Tadalafil Daily Compared With Tadalafil On-Demand in Treating Men With Erectile Dysfunction. Sex Med. 2019;7(3):282-291. DOI: 10.1016/j.esxm.2019.06.006. Concluded tadalafil daily provides a preferable therapeutic effect with a lower incidence of treatment-emergent adverse events relative to on-demand dosing over at least 24 weeks.
- Seftel AD, Goldfischer E, Kim ED, Dula E, Zeigler H, Burns P. Onset of efficacy of tadalafil once daily in men with erectile dysfunction: a randomized, double-blind, placebo controlled trial. J Urol. 2011;186(2):682-688. PMID: 21074803. Used tadalafil 5 mg once daily; significantly more men achieved successful intercourse than those on placebo by day 2 (48.6% vs 36.6%, p < 0.025).
Written by Teo Cho, health explainer. Last reviewed January 2026.
Shared to inform, not to treat. See a licensed clinician before starting a new medication.




